
High blood pressure
Read this even if you think your BP is fine
I have put together this guide to high blood pressure after a friend complained that the advice she received from her doctor and others was unclear. But you don’t need to have received a high blood pressure warning from your doctor to find this blog post interesting. In fact, some of the material may be most important for people who are not aware of what their blood pressure is, or who maybe complacently think that their readings are fine, when actually they are not. Some of this material certainly changed my view – from one of some detachment because I thought my results were good, to one of some concern that I should be trying to reduce my blood pressure.
The post covers:
What is high blood pressure
What is the evidence that high blood pressure is bad for one’s health
How should blood pressure readings be taken
Can various “lifestyle changes” reduce high blood pressure
Are the common medicines for high blood pressure worth taking
I have used the most credible sources available, including the NHS website, reports from the National Institute for Health and Care Excellence (NICE), the British Heart Foundation and various academic sources, mainly meta-analyses[1] and reviews.
What is high blood pressure?
Blood pressure is the amount of pressure inside your arteries. This pressure is necessary for your heart to pump blood. High blood pressure is when your blood pressure is higher than it should be, even when resting. It causes your heart to work harder to pump blood around your body. The medical name for high blood pressure is hypertension.
It is estimated that just over a quarter of adults in England had hypertension in 2017, with prevalence slightly higher in men than in women.
High blood pressure is partly genetic. Research on twins suggests that up to 40% of variability in blood pressure may be explained by genetic factors. So a positive family history increases the risk of developing hypertension. People of black African and black Caribbean origin are more likely to be diagnosed with hypertension. High blood pressure is also associated with social and lifestyle factors. People from the most deprived areas in England are 30% more likely to have hypertension than those from the least deprived. This is probably because social deprivation is often correlated with smoking, excessive alcohol consumption, excess dietary salt, unhealthy diet, obesity and lack of physical activity – all of which are associated with hypertension. Anxiety and emotional stress can also raise blood pressure.
Blood pressure readings are given as two numbers, with the first number higher than the second. This is what the two numbers are measuring:

If you’re under 80 years of age, you’re usually considered to have high blood pressure if your reading is either:
140/90 or higher when checked by a healthcare professional
135/85 or higher when checked at home
If you’re aged 80 or over, you’re usually considered to have high blood pressure if your reading is either:
150/90 or higher when checked by a healthcare professional
145/85 or higher when checked at home
The different thresholds, depending on whether the measurements are taken by a healthcare professional or done at home, are due to “white coat” syndrome, meaning some people tend to exhibit slightly higher blood pressure when a doctor or other medical professional takes their reading than when they measure their blood pressure themselves.[2] One review (p19) suggested that white coat syndrome may affect as many as 20–35% of patients diagnosed with hypertension.
The NHS website classifies blood pressure readings as shown below, assuming the reading was taken by a medical professional. The reading of 145/85, marked by the cross in the chart, is high.
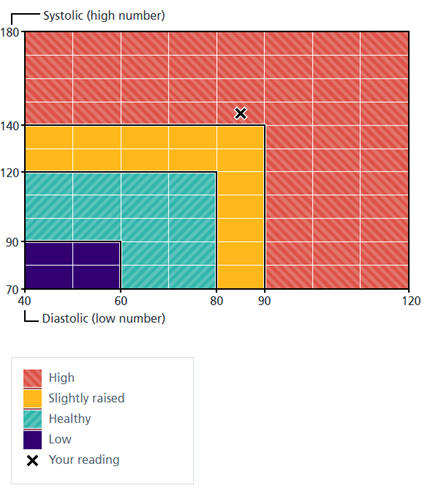
However, the British Heart Foundation uses a more nuanced breakdown, which in this case – a measurement of 145/85 – is also harder to interpret: the systolic figure is high (stage 1), but the diastolic figure is only “slightly raised”.

Confusingly, American healthcare guidance uses lower thresholds than we do in the UK[3]:

Using the lower US thresholds would effectively double the number of people defined as having high blood pressure:

Also note from the chart above that systolic blood pressure tends to increase with age.
Diastolic blood pressure on average increases with age up to around 50, then gradually falls again, meaning that systolic blood pressure is the major risk factor in older people.

What is the evidence that high blood pressure is bad for one’s health?
According to the NHS England website, high blood pressure “can increase your risk of serious conditions such as heart disease, heart attacks, strokes, heart failure, kidney disease and vascular dementia. Lowering your blood pressure even a small amount can help reduce your risk of these problems”.
Perhaps the best quality UK evidence about the size of these risks comes from a study led by academics from the University of London and published in The Lancet in 2014. It uses electronic health records of 1.25 million UK patients from 1997 to 2010, 30 years of age or older and initially free from cardiovascular disease, a fifth of whom were receiving blood pressure-lowering treatments. The study looks at the patients’ baseline blood pressure then their cardiovascular history over a period of around five years. Later blood pressure readings were not taken, nor did the study take account of any medications.
The research concluded that for a person aged 60 with hypertension, the lifetime risk of cardiovascular disease was around 60%, compared with around 45% for someone without high blood pressure.
High systolic blood pressure was particularly strongly associated with strokes (brain haemorrhages), with an increased lifetime risk of some 35-44% compared with someone with blood pressure of 115/75 (which was close to the mean for the study participants). There was a similar increased risk of angina (41%). For all twelve cardiovascular conditions in the study, the increased risk from having high systolic blood pressure was 26%.
In each age group, the lowest risk for cardiovascular disease was in people with systolic blood pressure of 90–114 mm Hg and diastolic blood pressure of 60–74 mm Hg. Above 130/85 mm Hg, “modest increases in either systolic or diastolic blood pressure were accompanied by large increases in hazard ratios” (i.e. the risk of having various cardiovascular diseases). But even with lower blood pressure levels, moving from the lowest group (90 – 114 mm Hg) to the next highest (115 – 129 mm Hg) greatly increased the risk, as the example below for angina shows.

The study found the same broad pattern for almost all the cardiovascular diseases studied – the only exceptions were cardiac arrest and intracerebral haemorrhage, where the lowest blood pressure group had very slightly higher risks than the 115 – 129 mm Hg group.
There is plenty of support from other studies for the findings that cardiovascular diseases increase in frequency with blood pressure readings even for people who do not have hypertension. Epidemiological data from the US Framingham Study, a very large and long-running piece of research, “showed that at all ages and in both sexes, cardiovascular risk increases incrementally with blood pressure, even within the normal range”. In the Framingham study, 45% of cardiovascular disease events in men occurred at a systolic blood pressure of lower than 140 mm Hg.
Researchers at Oxford University published a large-scale analysis of randomised trials in 2021, looking at the health impacts of medicines that reduce blood pressure. They found that a 5 mm Hg reduction of systolic blood pressure reduced the risk of major cardiovascular events by about 10%, irrespective of previous diagnoses of cardiovascular disease, and even at normal or high–normal blood pressure values (just over a quarter of participants had a systolic blood pressure of less than 130 mm Hg at the start of the trials).
An earlier 2015 meta-analysis led by Oxford University researchers found that every 10 mm Hg systolic blood pressure reduction reduced the risk of major cardiovascular events by 20%, coronary heart disease by 17%, stroke by 27%, heart failure by 28% and death from all causes by 13%. It, too, found that the proportional effects were similar in trials that included people with lower baseline systolic blood pressure (under 130 mm Hg). The researchers concluded that the results “provide strong support for lowering blood pressure to systolic blood pressures less than 130 mm Hg”.
In fact, as long ago as 2002 The Lancet published a meta analysis that concluded that “throughout middle and old age, usual blood pressure is strongly and directly related to vascular (and overall) mortality, without any evidence of a threshold down to at least 115/75 mm Hg”.
Evidence like this persuaded the US health authorities in 2004 (p11) to introduce a new classification that includes the term “prehypertension” for those with blood pressures ranging from 120–139 mm Hg systolic and/or 80–89 mm Hg diastolic. This category was subsequently split between “elevated” (120 -129 mm Hg systolic) and “stage 1 hypertension” (130 – 139/80 – 89 mm Hg).
In the UK, medical practice seems to have ignored the large body of very credible evidence about the health risks of raised blood pressure. In particular, NICE is very cautious about recommending blood pressure medication. For stage 1 hypertension (clinic blood pressure reading between 140/90 mm Hg to 159/99 mm Hg), NICE only advises doctors “discuss starting antihypertensive drug treatment, in addition to lifestyle advice, with people aged under 80 years”, when the hypertension is “persistent” and the patient also has “one or more of the following: target organ damage, established cardiovascular disease (CVD), renal disease, diabetes, an estimated 10-year risk of CVD of 10% or more”. For patients under 60 with an estimated 10-year risk of CVD under 10%, again NICE only recommends considering drug treatment.
So the health risks of high blood pressure are significant. But perhaps the main take-away from the research is that the official UK thresholds for hypertension – for example, for people aged under 80, 140/90 mm Hg or higher when checked by a healthcare professional – are too high and may well be misleading. There are clear health benefits in having much lower blood pressure than the 129/83 mm Hg, for example, which the British Heart Foundation guidance would describe as “healthy”. And NICE’s guidance would definitely not see doctors advising patients that they could usefully reduce their blood pressure further, even if it was close to 140/90 mm Hg.
How should blood pressure readings be taken?
The diagram below gives a typical explanation of how to measure your blood pressure at home.

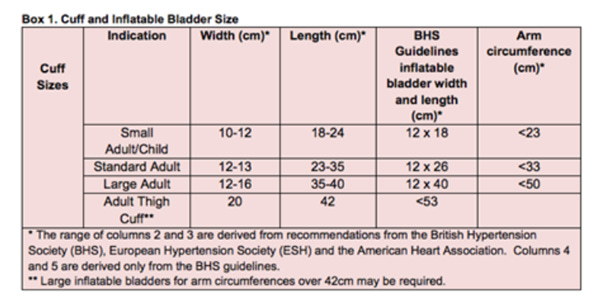
It’s important to use a machine that is clinically validated, so the results are accurate and reliable. Here’s a link to suitable machines. You need to make sure that the cuff fits your arm, especially if you are not an average size.
The British Heart Foundation and others recommend getting your device serviced by the manufacturer every two years or so. Realistically, it would be cheaper to buy a replacement in most cases.
It’s also a good idea to measure blood pressure in both arms, at least initially, as large differences in systolic pressure are linked to much higher cardiovascular risk than if readings are very similar. If there is a difference in readings, but it does not seem high enough to raise with your doctor, you should take readings from the arm with the higher reading in future.
The general advice is to take two or three readings, each about one to two minutes apart. If your first reading is much higher than the next, ignore it and take an extra reading.
NICE advises that blood pressure measurements should be taken twice daily, ideally in the morning and evening and continue for at least four days, and ideally for seven days. They also suggest discarding the measurements taken on the first day and using the average value of all the remaining measurements. However, there seems to be no material effect on results from discarding the first day measurements or measuring beyond five days, according to Oxford University’s Centre for Evidence-Based Medicine (CEBM).
CEBM research also found that patients taking their own readings “produced on average a higher (around 7 mm Hg) blood pressure when compared with 24 hour ambulatory monitoring”,[4] meaning that half the participants were incorrectly diagnosed as having hypertension when they didn’t. The figures were even worse for GP measured blood pressure. So if your own or your doctor’s readings look to be marginal, NICE (para 1.2.3) recommend 24 hour ambulatory monitoring for a day to get a more accurate result: “If clinic blood pressure is between 140/90 mmHg and 180/120 mmHg, offer ambulatory blood pressure monitoring (ABPM) to confirm the diagnosis of hypertension”.
Blood Pressure UK suggests that once you have a record of your blood pressure over a week, “you can take readings less often – once every one to two weeks perhaps. Your doctor or nurse can talk to you about this, there’s no need to measure it too often. If your blood pressure has been stable for a long time, you might only need to measure it once every four to six months. Your doctor or nurse will be able to advise you”.
Can lifestyle changes reduce high blood pressure?
If you have high blood pressure, your doctor is very likely to review various “lifestyle changes” with you to see if these might lower it. Some of these changes may be more effective than others. I’ve set out below what the evidence says, grouping them into strongly recommended, recommended and not recommended, based on my personal assessment of the research.
Strongly recommended
Reducing weight is widely advised as a way of reducing blood pressure. A large scale study in the UK looked at individuals with what is regarded as a normal weight (body mass index, BMI, of 18.5–24.9 kg/m2), compared with groups who were overweight (BMI 25.0–29.9 kg/m2 ) and of varying degrees of obesity (BMI up to 45.0 kg/m2).

The most obese people had a more than threefold higher risk of hypertension compared with the normal weight reference group. Even the overweight group had a significantly higher risk of hypertension. So losing weight if you are clinically overweight or obese is probably the best thing you can do to reduce your blood pressure.
Doing (more) exercise is also widely recommended. A 2016 meta-analysis found that research supported this advice. The average effect size was a reduction of nearly 5 mm Hg for systolic blood pressure and just over 3 mm Hg for diastolic. The reductions were statistically significant regardless of the participant’s initial blood pressure level, gender, physical activity level, antihypertensive drug intake, type of blood pressure measurement and type of exercise performed. However, reductions were greater if participants were males, not receiving antihypertensive medication, physically active and if the exercise performed was jogging. But there were still positive benefits for other aerobic exercises such as walking, cycling, or a combination of these, as well as for conventional or circuit resistance training exercise.
Reducing salt intake is often suggested as a possible means of reducing blood pressure. There is good evidence to support this recommendation. A 2013 review and meta-analysis looked at thirty four trials where participants reduced their salt intake. The average change in urinary sodium was equivalent to a reduction of 4.4 g of salt/day and with this reduction in salt intake, the mean change in blood pressure was just over 4 mm Hg for systolic blood pressure and 2 mm Hg for diastolic. The average person in the UK is thought to eat around 8.1g salt a day, compared with a government target of 6 g/day. The review authors argue that achieving the 6 g/day target would “have a major effect on blood pressure, but a further reduction to 3 g/day will have a greater effect and should become the long term target for population salt intake”.
Recommended
Other research has looked at the benefits of increasing potassium consumption, either through dietary changes or taking potassium supplements (between 60 - 100 mmol/day). A meta-analysis showed that increased potassium intake led to a reduction of around 3 and 2 mm Hg in systolic and diastolic blood pressure respectively.[5] Another study found that women with the highest amount of potassium in their diet had an 11 per cent lower risk of having a heart attack or stroke, compared to women with the lowest amount of potassium. For men with the highest amount of potassium, the risk was 7 per cent lower. Potassium-rich foods include avocados, bananas, salmon, broccoli and spinach.
Reducing alcohol intake is also widely recommended. However, a recent meta-analysis found no significant effect on blood pressure from reducing their consumption for people who drank two or fewer units per day. The effect only applied in people who drank more than two units per day, with the effect being strongest in participants who drank six or more units per day if they reduced their intake by about 50%. Their systolic blood pressure fell by 5·5 mm Hg on average (and nearly 4 mm Hg for diastolic).
Various specific foodstuffs have been examined to see if they affect blood pressure. Of these, there is reasonable evidence that drinking 250ml of beetroot juice a day can reduce high blood pressure, probably by around 7.5/3 mm Hg. The obvious limitation of this research was that only 68 people participated in the trial, of whom half were in the control group. Nevertheless, the results were statistically significant and the research design – a randomised, blind trial – is a very good one.
More generally, eating a healthy diet is also widely recommended. There is some evidence to support this advice. For example, a 2016 meta-analysis found that the DASH (Dietary Approaches to Stop Hypertension) diet and Nordic diet lowered systolic blood pressure by just over 4 mm Hg (and just over 2 mm Hg for diastolic). These diets are rich in fruit, vegetables, whole grains, legumes, seeds, nuts, fish and dairy and low in meat, sweets, and alcohol. However, there are a couple of caveats with this research, notably that some of the studies included low alcohol consumption as part of the diet, so it is not clear to what extent improvements were due to the food consumed or the alcohol not consumed. Some of the studies did not directly control what people ate and the studies were generally for relatively short periods – up to six months.
Not recommended
Relaxation programmes, such as mindfulness and meditation, have also been recommended to reduce blood pressure. There is some evidence that mindfulness can reduce blood pressure, but the trials used are not very high quality, with one recent meta-analysis noting that the trials examined “exhibited a noticeable selection and publication bias” [i.e. unsuccessful trials appeared less likely to be reported], and other limitations “included a small sample size, discrepancies in type, duration, and dosage of [mediation therapies] and lack of long-term follow-up”. NICE deleted its recommendation on relaxation in its most recent guidelines on blood pressure, noting that “It is not the intention of the committee to stop people from trying relaxation therapies if they wish to, but to make people aware that there is less evidence for benefit of this intervention compared with other lifestyle interventions or pharmacological treatment”.
Stopping smoking is also widely advised as a means to reduce blood pressure.[6] The act of smoking does temporarily increase blood pressure – known as an acute effect. But the evidence that smoking increases underlying blood pressure - has a chronic effect - is not strong. A large scale study in England from the mid-1990s found that “overall, age-adjusted blood pressures did not differ importantly among never, past, and current smokers”. In men, non-smokers’ average systolic blood pressure was under 1 mm Hg lower than that of current smokers and less than 2 mm Hg lower than for heavy smokers. In women, the lowest results were observed among light smokers, who had slightly lower levels than never smokers. Another study from China found a substantially greater risk of high blood pressure in men who had stopped smoking than in current smokers. A more recent review described the evidence on the link between smoking and high blood pressure as “inconclusive”, noting that increases in blood pressure of people who stop smoking may be due to their increased weight – a common effect in such cases – rather than anything directly related to nicotine.
Reducing caffeine consumption is also widely recommended. One recent review states that it is widely agreed that blood pressure generally increases 30 minutes after caffeine consumption, reaches a peak after 60–90 minutes and returns to baseline after about 2 to 4 hours. However, “the relationship between habitual caffeine intake and long-term changes in [blood pressure] … are conflicting and difficult to interpret because the data on clinical effects are mixed: equivocal, null and positive”.
Are the common medicines for high blood pressure worth taking?
One commonly recommended type of drug to reduce blood pressure are ACE inhibitors.[7] These are one of the first treatments recommended by NICE for people with high blood pressure. A recent meta-analysis found that these drugs have a “modest” effect, reducing systolic pressure by around 8 mm Hg for (5 mm Hg for diastolic pressure), compared with a placebo. Most of the blood pressure lowering effect (about 70%) can be achieved with the lowest recommended dose of the drugs and 90% of the maximum effect can be achieved with half the maximum dose. They found that “no ACE inhibitor drug appears to be any better or worse than others in terms of blood pressure lowering ability”.
Probably the main alternative to ACE inhibitors are calcium channel blockers (CCBs)[8], which NICE also recommends. A 2017 review concluded that “for [blood pressure] lowering, CCBs were at least as efficacious as comparators. The findings of our systematic review and analysis add to the body of evidence for the use of CCBs for the long-term treatment of hypertension in difficult-to-treat high [cardiovascular] risk populations”.
I’ve not looked at other medicines or at side-effects. Suffice to say that all medicines potentially have side-effects, but from what I’ve seen these are no more of an issue with hypertension drugs than with other medications.
NICE notes that “a single antihypertensive drug is often inadequate in the management of hypertension, and additional antihypertensive drugs are usually added in a stepwise manner until control is achieved”. They set out four stages, with an additional drug being added in each if the previous drug regime was unsuccessful in bringing blood pressure “under control”, meaning a patient has persistently elevated blood pressure despite the use of two or more medications. In fact, there is recent evidence that taking three or four medications at lower doses, rather than just a single pill, may help people lower their blood pressure without increasing the risk of most negative side effects. “People treated with low-dose drug combinations saw their systolic blood pressure decrease on average by 16 to 28 mm Hg over four to 12 weeks, the analysis showed. In contrast, systolic blood pressure decreased 12 to 18 mm Hg on average in the group taking one drug or receiving usual care”. However, these results were based on only five trials and under 2,000 patients, so ideally they should be confirmed by more and larger trials.
In future, patients may also be prescribed a new drug, baxdrostat, which in clinical trials has reduced blood pressure by about 9-10 mm Hg more than a placebo, with about four in ten patients taking the drug reaching “healthy” blood pressure levels, compared with fewer than two in ten on the placebo. The principal researcher said “I’ve never seen blood pressure reductions of this magnitude with a drug”. Baxdrostat works by reducing the body’s over-production of the hormone aldosterone, which can cause the body to hold on to salt and water and thereby push up blood pressure.
It has been suggested that taking medication just before going to bed may be more effective, but other trials have not found support for this idea and the results have been questioned by other researchers.
Some conclusions
My main conclusions from reading the literature are:
High blood pressure definitely has health risks that most people would want to reduce;
Don’t worry too much about the precise blood pressure readings you get: with different ways to measure blood pressure there are bound to be variations and the official UK hypertension thresholds are pretty arbitrary and almost certainly too high;
Even if your blood pressure reading is well below what is defined as hypertension in the UK, there are still significant health benefits from trying to reduce it further;
The best way to reduce blood pressure without taking medications is to lose weight if you are clinically overweight or obese, but more exercise and reducing salt intake are also strongly recommended and should benefit everyone, as would cutting alcohol consumption if you’re a heavy drinker. A healthier diet with more potassium should help. Don’t stop smoking or drinking caffeine or start doing relaxation therapies to reduce blood pressure – there’s not enough evidence they work;
If your doctor suggests you take medication to reduce your blood pressure, follow their advice. Relatively small doses – no more than half the maximum – deliver disproportionate reductions. It may be desirable, or even necessary, to take two or three different medicines to achieve a substantial reduction – this is not uncommon or anything to worry about unduly.
[1] A meta-analysis pools results from previous quantitative research on a topic in order to identify the main trends. If well conducted, it should generate more credible results than any one individual piece of research.
[2] One review concluded that “the white coat phenomenon is a common, periodic, neuro-endocrine reflex conditioned by anticipation of having the blood pressure taken and the fear of what this measurement may indicate concerning future illness. It does not change with time or with prolonged association with the physician”. It also noted that “The effect is essentially systolic”, i.e. the first, higher number is likely to increase much more than the second, lower number when blood pressure is measured by a medical professional.
[3] The World Health Organisation also recommends using the 140/90 threshold that is applied in the UK when considering giving medicines for hypertension, as do the health authorities in Australia (p32) and Europe (p13). Canada applies the same 130/80 threshold as the US and Japan lowered its guidance to these levels in 2019. So the picture is not clear!
[4] 24 hour ambulatory monitoring involves wearing a device that automatically takes measurements two to three times an hour (once per hour at night). This is currently considered the “gold” or reference standard for diagnosing high blood pressure, according to CEBM.
[5] These figures exclude one outlier which significantly increased the effects.
[6] To be clear, I’m not recommending that anyone should stop smoking as a means to reduce their blood pressure, as there is no strong evidence it would have any great impact. But there are other obvious health reasons to stop smoking.
[7] According to the British Heart Foundation, “ACE inhibitors can reduce the activity of an enzyme called angiotensin-converting enzyme, or ACE for short. The enzyme is responsible for hormones that help control your blood pressure. It has a powerful narrowing effect on your blood vessels, which increases your blood pressure. ACE inhibitors inhibit or limit this enzyme, making your blood vessels relax and widen. This, in turn, lowers your blood pressure and improves blood flow to your heart muscle”.
[8] According to the British Heart Foundation, CCBs reduce the amount of calcium entering cells of the heart and blood vessel walls. This is significant because calcium is necessary to contract the muscular linings of blood vessels throughout your body (for example, the arteries that supply your heart with oxygen). As a result, the blood vessels relax and the heart muscle receives more oxygenated blood, which is how CCBs are able to lower blood pressure and treat angina. CCBs therefore work on a different mechanism than ACE inhibitors to reduce blood pressure.